





Clinical development planning is changing as global sponsors look for trial locations that can offer speed, quality, scientific depth, and regulatory confidence together. For many years, India was discussed mainly as a cost-efficient clinical trial destination. Cost still matters, but it is no longer the main story. The stronger story is that India is becoming a serious clinical development partner for global pharma and biotech companies that need scalable global clinical trials, integrated clinical development, strong global clinical operations, and reliable execution from early development to submission.
This shift has gradually come through better clinical infrastructure, stronger investigator experience, more organized hospital networks, improved regulatory systems, wider use of digital trial tools, and growing experience in global studies. The result is important: India can support clinical programs not only as an execution location, but as a strategic part of global development planning.
For sponsors, this matters because clinical development is under pressure. Pipelines are more complex. First-in-human studies are more demanding. Advanced therapies and specialty assets need careful safety oversight. Patient recruitment remains difficult in many mature markets. Data packages must meet global expectations. Regulatory submissions need consistency across clinical operations, safety, biostatistics, data management, and medical writing.
In this setting, India’s value is not just that trials can be run here. The real value is that India can help sponsors move development programs forward with better coordination, faster recruitment, and stronger scientific and operational control.
Beyond cost: clinical development planning with India in the strategy
The old India story was simple: large patient population, lower cost, and available sites. That story is incomplete now. It misses the deeper change taking place in Indian clinical research.
India today offers a combination that many global sponsors need. There is a large and diverse patient population, including treatment-naïve patients across areas such as oncology, metabolic disease, infectious disease, and inflammatory disorders. There is also a more mature base of GCP-compliant sites, experienced investigators, clinical research professionals, regulatory teams, data managers, statisticians, and medical writers.
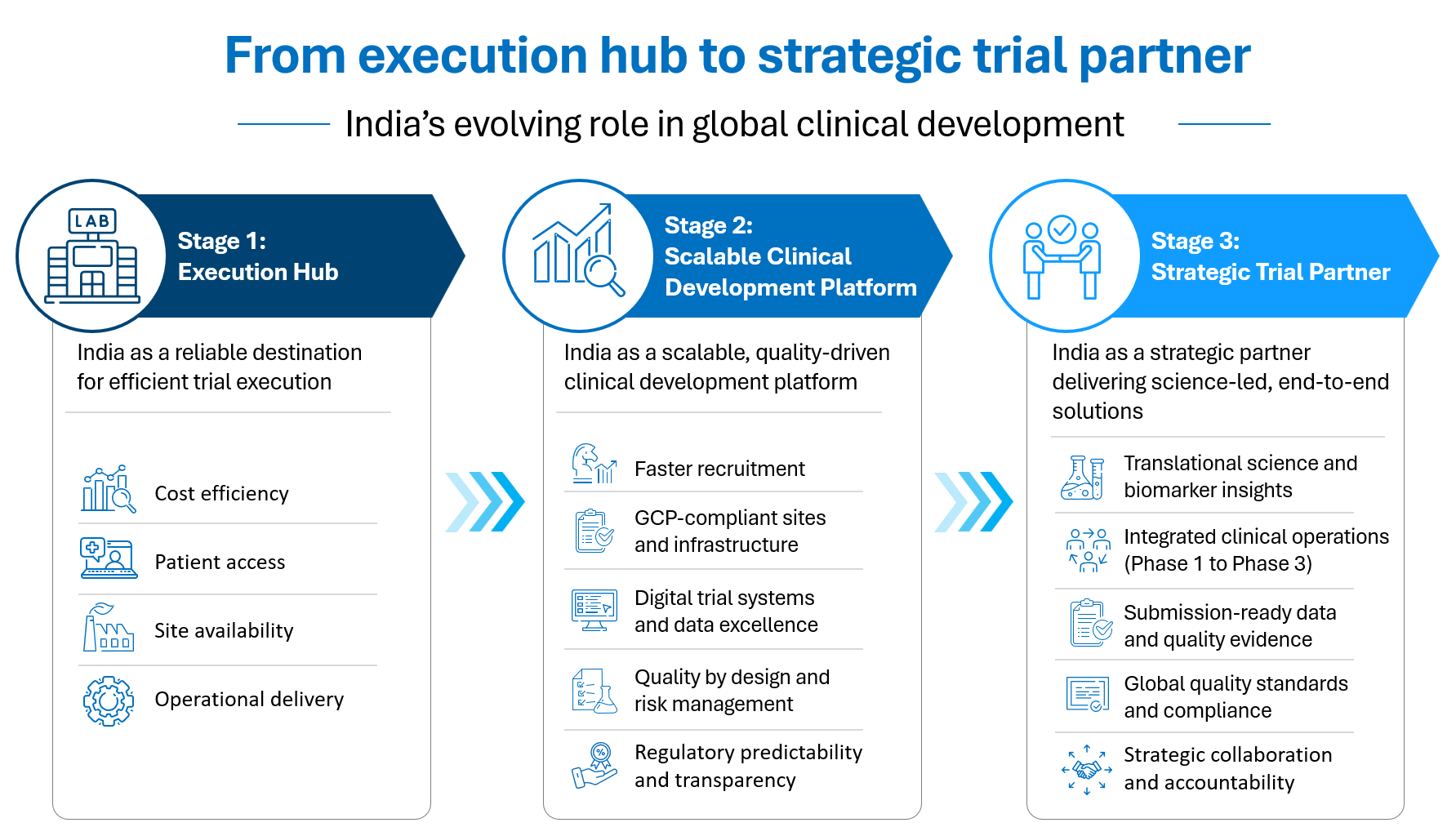
Figure 1. India’s clinical development value is shifting from cost-led execution to scalable, integrated, and science-led partnership.
This combination of speed, scale, regulatory improvement, clinical infrastructure, and treatment-naïve patient access gives India a stronger position in global clinical development. It moves India away from being seen as a low-cost option and toward being seen as a development partner that can support global trial strategy.
This distinction matters. A low-cost location is replaceable. A strategic development partner is not.
Why global clinical trials need speed with quality control
Recruitment delays remain one of the biggest problems in clinical development. Many studies lose time because patient identification is slow, site activation is uneven, or competing trials make enrollment difficult. In this area, India has a clear advantage when the trial is planned properly.
India offers large disease pools, high patient throughput in many centers, and the ability to recruit across multiple cities in parallel. This can help sponsors recover time, especially in Phase II and Phase III programs where recruitment volume becomes critical.
However, speed alone is not enough. Poorly managed speed creates risk. Fast enrollment means little if data quality is weak, protocol deviations increase, or safety monitoring is not strong enough. That is why the better message is not simply that India is fast. The sharper message is that India can be fast when recruitment, site selection, quality systems, data flow, and oversight are built properly from the start.
India’s speed advantage depends on globally harmonized protocols, careful site selection, early regulatory planning, strong documentation, clinical development planning, and a clear understanding of local regulatory expectations. Without these, the advantage can quickly disappear. Sponsors need more than access to sites. They need global clinical operations that can connect sites, safety, data, science, and submission planning.
Regulation is becoming more predictable
For global sponsors, regulatory predictability matters as much as patient access. If regulatory pathways are unclear, timelines become difficult to plan. Sponsors hesitate to include a country in global trials if they cannot estimate approval routes, documentation expectations, or ethics committee requirements.
India has made important progress here. The New Drugs and Clinical Trials Rules, 2019 created a more structured framework for clinical trial approvals. The roles of CDSCO, Subject Expert Committees, and ethics committees have become clearer. The linkage between regulatory approval and ethics oversight has also become more defined.
India’s regulatory environment has moved toward a more rule-driven system, with stronger alignment to global expectations such as ICH-GCP, CTD formats, and benefit-risk thinking. This does not mean every problem has disappeared. No serious discussion should pretend that. Some timeline variability still exists. Certain query responses may not always follow fixed statutory timelines. There are still areas where India differs from the US and Europe in review depth, process transparency, and post-approval requirements.
But the direction is clear. India is no longer operating in an unclear or loosely structured clinical trial environment. It is moving toward a more predictable and globally recognizable regulatory system. For sponsors, this improves planning confidence. It also makes India easier to include in global development strategies, especially when the partner understands both Indian regulatory expectations and global submission standards.
The rise of integrated clinical development
The real change in global trials is not only geographical. It is structural.
Clinical development is becoming too complex for fragmented execution. Sponsors often work with multiple vendors: one for clinical operations, one for data management, one for biostatistics, one for medical writing, one for bioanalysis, one for safety, and another for regulatory support. This can work, but it also creates risk.
The risk is not always technical. It is often organizational. Different vendors may use different standards, timelines, templates, assumptions, and communication processes. One team may update the statistical outputs while another is preparing the clinical study report. One vendor may record laboratory data in one format, while another uses a different convention. Safety narratives may not fully match the final datasets. These small mismatches become serious in the final weeks before submission.
This is why integrated clinical development models are becoming more valuable. Sponsors need partners who can connect clinical operations, bioanalysis, data management, biostatistics, pharmacovigilance, medical writing, quality assurance, and regulatory support in one coherent operating model.
Syngene’s TnCR model fits this direction. It brings together translational services, clinical operations, medical writing, data management, programming, biostatistics, bioanalysis, pharmacovigilance, medical monitoring, quality control, quality assurance, and project management. That breadth is useful only if it is coordinated. Many companies can list many services. The stronger point is that integrated delivery reduces handoffs, improves accountability, protects data consistency, and helps sponsors move from clinical conduct to submission with fewer avoidable gaps.
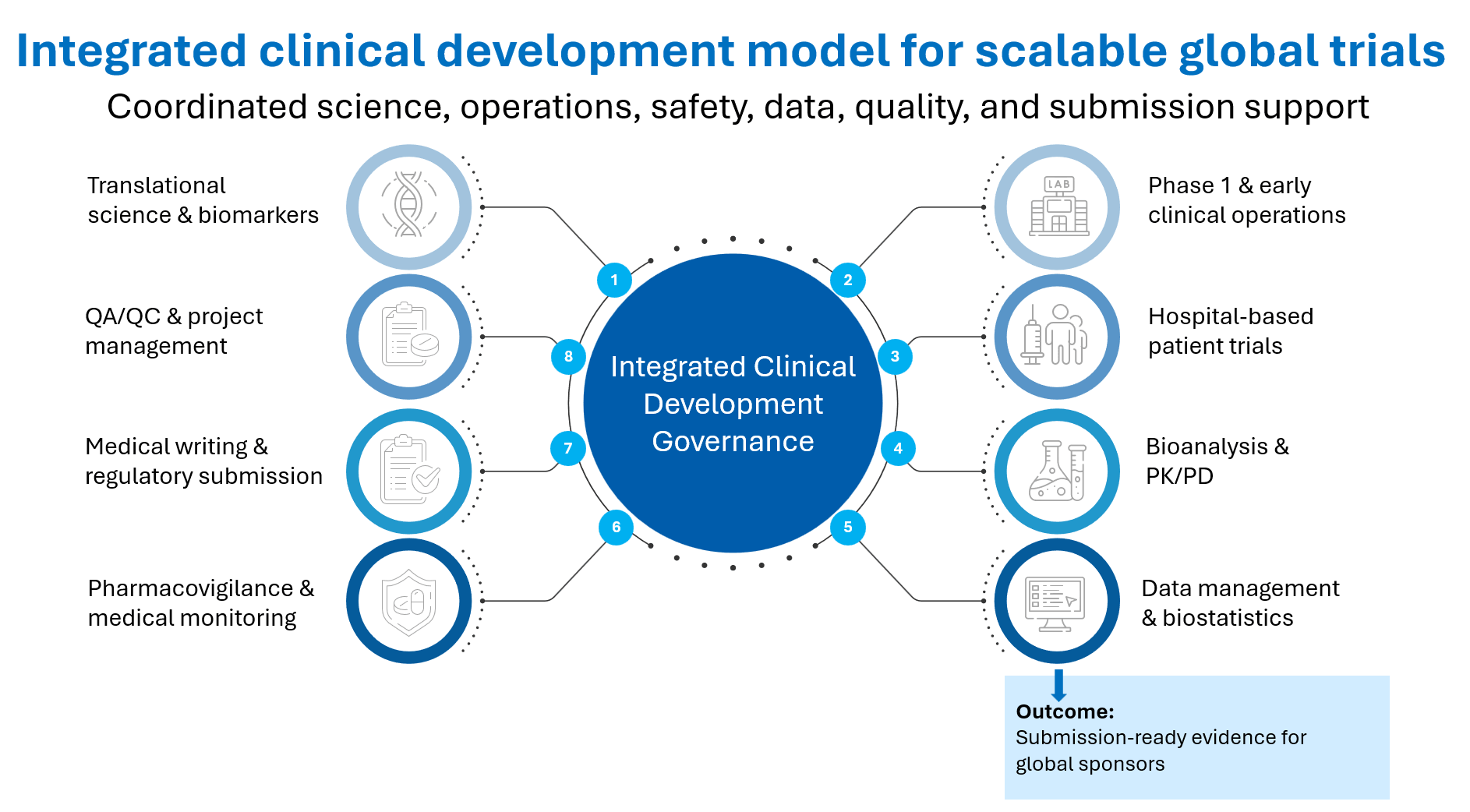
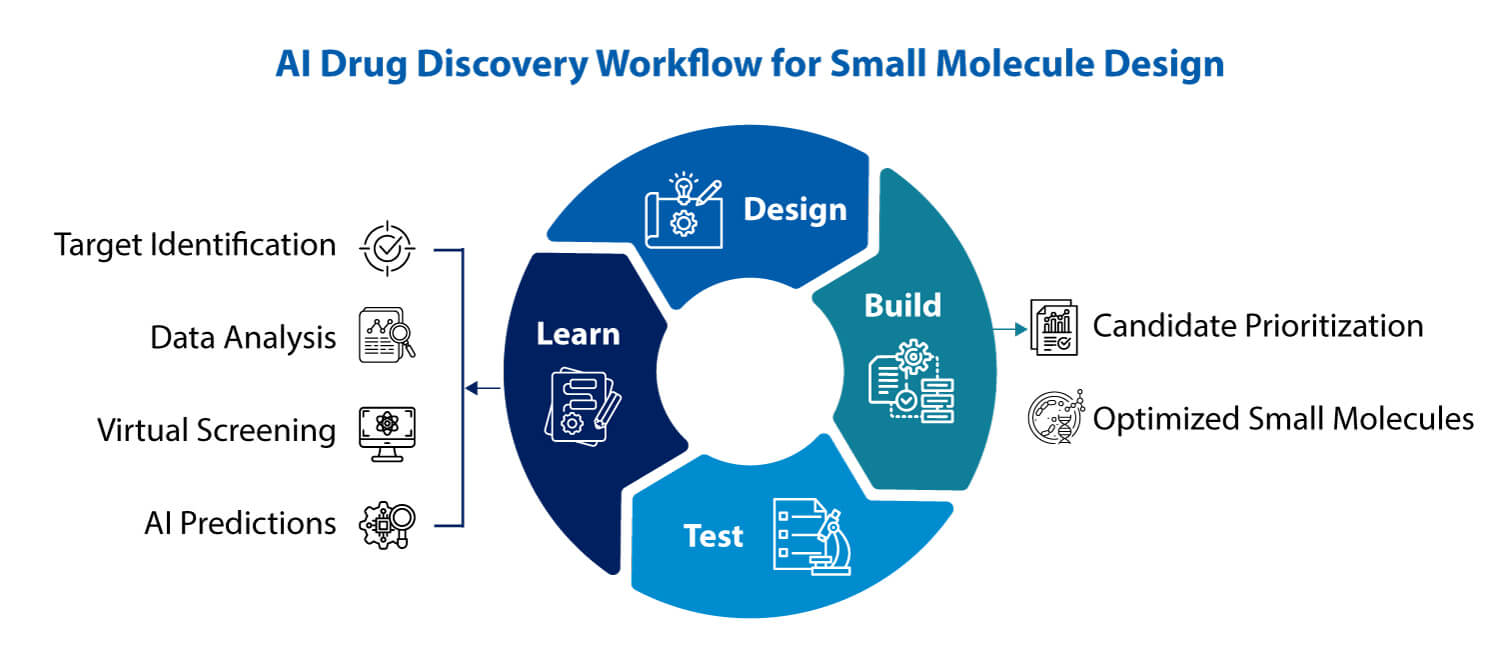
Figure 2. Integrated clinical development connects science, operations, safety, data, quality, and submission support under one accountable model.
PK PD bioanalysis and translational science give India a sharper role
India’s next role in clinical development will not be built only on enrollment. That would be a weak and limited position. The more differentiated role will come from combining patient access with translational science.
Early development is where many programs fail. A compound may look promising in preclinical models, but the same promise may not translate into humans. This is especially difficult in first-in-human and proof-of-concept studies, where sponsors need early evidence of safety, target engagement, dose response, and biological activity.
Biomarkers are critical in this setting. They help confirm whether the therapy is reaching the intended target. They can provide early signals of pharmacodynamic activity. They can guide dose escalation and dose selection. They also help sponsors make better go/no-go decisions before committing larger investments.
This is where integrated clinical development becomes important. PK/PD thinking, biomarker strategy, bioanalysis, and clinical execution cannot sit in separate lanes when early development decisions depend on how these signals come together. A clinical development partner that can connect discovery, preclinical evidence, PK/PD thinking, biomarker strategy, bioanalysis, and clinical execution is more valuable than a partner that only runs trial operations.
This is especially relevant for global biotech companies. Many smaller and mid-sized biotechs have strong science but lean internal teams. They may need a partner who can help them interpret early development signals, not merely execute a protocol. This is where India can become more than a recruitment location. It can become part of the scientific decision-making system.
Global clinical operations need hybrid execution models
First-in-human and complex early-phase trials are becoming more demanding. Many new assets involve novel mechanisms, narrow safety margins, intensive PK/PD sampling, biomarker analysis, and, in some cases, patient dosing from the first administration.
A traditional Phase 1 unit may offer strong operational control, but it may not always have access to the right patient population or disease-area specialists. A hospital may offer clinical expertise and patient access, but may need additional support for Phase 1 governance, dense sampling schedules, safety oversight, and protocol discipline.
This is why hybrid execution models are becoming important. A Phase 1 unit and tertiary hospitals can complement each other. The Phase 1 unit brings discipline, controlled processes, safety monitoring, PK operations, and study execution systems. Hospitals bring specialist physicians, disease-area knowledge, patient access, and infrastructure for managing higher-risk clinical situations.
This is a strong, practical story for Syngene. It does not sound like marketing decoration because it addresses a real sponsor problem: how to run complex early-phase trials safely and efficiently when the study needs both operational control and clinical depth. Syngene’s ability to conduct healthy volunteer studies in-house under controlled conditions, while also supporting patient-based trials through hospital collaborations, gives this model practical relevance.
Digitalization, data flow, and global clinical supply reliability
Digital tools are also changing India’s clinical trial value proposition. Electronic source systems, real-time data capture, integrated lab and clinical platforms, risk-based monitoring, electronic patient-reported outcomes, wearables, and continuous monitoring devices can improve data quality and reduce manual errors.
The value is not that digital tools sound modern. The value is that they reduce friction in trial execution. They help investigators see safety signals earlier. They reduce paperwork. They support faster data review. They improve traceability. They can also make participation easier for patients.
This is another area where India can strengthen its position. If India combines patient access with digital trial infrastructure, the country can support faster and more reliable clinical development. But this requires discipline. Digital tools do not fix poor processes. They work only when protocols, data standards, site training, and governance are already strong.
The China-plus-one question
Many sponsors are reassessing global development geographies. China remains an important market and development location, but sponsors are also looking for diversification. India is naturally part of this discussion.
The China-plus-one argument should be handled carefully. India should not position itself only as an alternative to China. That is reactive. The stronger argument is that India has its own clinical development strengths: English-speaking scientific talent, large and diverse patient access, improving regulation, strong hospital networks, growing digital maturity, and experience with global quality expectations.
This gives India a practical advantage for sponsors who want more resilience in their clinical development footprint. But the message should not be that India will replace China. That would be simplistic and easy to challenge. The better message is that India can become a credible, high-quality development geography for sponsors who want more patient access, more flexibility, and more optionality in global clinical programs.
What global sponsors should look for
The next stage of global clinical development will reward partners who can reduce complexity. Sponsors should not only ask whether a provider can run a study. They should ask harder questions.
Can the partner support early scientific translation? Can it handle biomarker strategy and bioanalysis? Can it run controlled early-phase studies and patient-based trials? Can it manage hospital networks? Can it support SDTM, ADaM, TLFs, clinical study reports, safety narratives, and eCTD-ready documentation? Can it build quality into the study instead of treating quality as a final inspection activity? Can it operate globally through partnerships while still maintaining accountability?
These are the questions that separate vendors from strategic partners.
India is now better placed to answer these questions than it was a decade ago. The infrastructure is stronger. The regulatory system is more structured. Investigator and site maturity has improved. Digital tools are becoming part of routine execution. Integrated service models are emerging.
For Syngene, the opportunity is clear. The company should not present itself merely as a CRO that can conduct trials from India. The stronger position is that Syngene can act as an integrated clinical development partner, connecting translational science, early-phase execution, patient trials, bioanalysis, data standards, safety, medical writing, and submission support within one accountable ecosystem.
India’s next role in global clinical development will not be defined by cost alone. It will be defined by how well the country can combine scientific judgment, patient access, operational rigor, digital reliability, regulatory alignment, and submission-quality evidence.
That is the real shift: from execution hub to strategic trial partner.