




Why this comparison matters for human dose prediction
Allometric scaling is one of the familiar starting points in human dose prediction, especially when teams have useful animal pharmacokinetic data but no clinical exposure data yet. Before a molecule reaches the clinic, teams need a reasonable sense of likely human exposure, the level of uncertainty still sitting in the data, and how confidently they can justify a starting dose and dosing plan. In this context, two well-established approaches are commonly considered: allometric scaling and physiologically based pharmacokinetic, or PBPK, modeling. Both are valuable tools for dose prediction, but they serve different purposes and are not interchangeable.
In many programs, the primary challenge is not the absence of a suitable model, but the inappropriate use of one. Simple methods are sometimes stretched beyond their intended scope, while more mechanistic approaches may be applied without sufficient supporting data. At times, these methods are presented as mutually exclusive, when in reality they are often complementary. The key question, therefore, is not which approach appears more sophisticated, but which is most appropriate for the specific decision being made.
What allometric scaling does with in vivo data
Allometric scaling is one of the standard ways of estimating human pharmacokinetics from animal data. It uses observed PK parameters from preclinical species and scales them to humans, mainly on the basis of body size or body weight differences across species. In development work, this is often done using parameters such as clearance and/or volume of distribution from animal studies and applying mathematical scaling relationships to estimate likely parameters in humans.
The attraction of allometry is obvious. It is direct, familiar, and practical. It is built on measured in vivo data, which gives it a strong place in early translational work. And when the relationship across species is reasonably consistent, it can provide a useful first estimate of likely human PK. This is important because not every program needs a highly detailed mechanistic model at the very beginning. In some cases, a sensible estimate from good animal data is exactly what the team needs to start shaping the clinical path.
Why allometry still has value
It is often assumed that allometry is too simple for modern development. That is not entirely justified. Allometric scaling continues to be used because it addresses a fundamental need in early translation. It gives teams an early translational estimate without demanding the large input package that PBPK usually needs. It can be applied relatively quickly. It is also grounded in actual preclinical observations rather than only in mechanistic assumptions.
In day-to-day development work, programs often need a practical starting point before they need a fully layered mechanistic explanation. A straightforward human PK estimate, even if it is imperfect, may still be very useful when teams are trying to compare molecules, shape early thinking, or sense-check broader development expectations.
In some situations, allometry can also reflect real in vivo behavior more naturally than a poorly informed mechanistic model. A simpler model built on strong data may be more helpful than a more elaborate model built on uncertain assumptions.
Where allometric scaling starts to become limited
The limitations of allometry usually become clearer when the biological question becomes more demanding. As allometric scaling is based mainly on size-related scaling, it assumes that the key biological processes are sufficiently similar across species for that scaling to make sense. That assumption can become uncomfortable quite quickly. Species differ in metabolism, transporter activity, absorption, protein binding, and formulation handling. Once those differences begin to matter, scaling by size alone may no longer carry enough explanatory weight. However, species-dependent scaling factors can correct the predicted parameters in some situations.
Allometry is also less useful when teams need to look beyond plasma PK. It does not naturally address tissue exposure, organ/tissue exposure, disease-related physiological changes, or complex situations such as drug-drug interactions and route-specific absorption differences. Those are not side questions in development. They often become central questions as a program moves closer to the clinic.
This does not mean allometry fails. It means it has a natural boundary. It is strong as a scaling approach, but it is not designed to answer every mechanistic question that follows.
What PBPK does differently as a mechanistic model
PBPK works on different principles. Rather than mainly scaling by body size, it tries to build a mechanistic picture of the drug profile using anatomy, physiology, and compound-specific properties. The body is represented through real organs and tissues, and drug movement is linked to factors such as organ blood flow, tissue volume, enzyme and transporter expression, lipophilicity, ionization, protein binding, permeability, route of administration, and formulation types.
This changes the kind of question the model can address. Allometric scaling is often useful when the question is, “Given the animal PK we have, what may the human value look like?” PBPK becomes more useful when the question is, “How may this drug behave in humans under a particular physiological condition, in a specific tissue, in a special population, or in the presence of an interacting drug?” This is an important difference. One gives a scaled estimate; the other gives a more biologically grounded argument.
Where PBPK adds real value in human dose prediction
PBPK becomes especially useful when the development question depends on more than a cross-species extrapolation.
When physiology matters
If the decision depends on organ blood flow, tissue composition, enzyme abundance, transporter effects, or route-specific absorption, PBPK has a clear advantage. Those factors can be built into the model directly rather than being left outside the frame. This makes PBPK particularly useful when the biological situation is complex, and the team needs more than a broad estimate.
When tissue exposure matters
One of the major differences between PBPK and allometry is that PBPK is not limited to plasma exposure. It can also support thinking about tissue PK. This can matter a great deal. In some programs, plasma concentration is a reasonable proxy for what the team needs to know. In others, it is not enough. Teams may need to understand exposure at the site of action, in an organ where toxicity is a concern, or in tissues where efficacy depends on local drug levels rather than on systemic concentration alone. PBPK gives a way to think about those questions more directly.
When special populations matter
PBPK is also more useful when the team needs to go beyond the standard healthy adult setting. Pediatrics, older adults, pregnancy, obesity, hepatic impairment, renal impairment, and disease-related physiological change all complicate dose prediction. These are exactly the kinds of situations where size-based extrapolation starts to show its limits. Because PBPK is built on physiology, it gives teams a better way to think through how altered biology may affect exposure and dose.
When DDI risk matters
Drug-drug interaction assessment is another area where PBPK brings clear value. Once metabolism, transport, or co-administered inhibitors and inducers come into the picture, a purely scaling-based approach is no longer enough. A mechanistic model becomes much more useful because it helps teams think through pathway contribution and likely exposure changes before those questions turn into clinical complications.
Why PBPK is not automatically the better choice
It is still a mistake to assume that PBPK should replace allometry by default. PBPK models are more demanding. They require expertise, good-quality inputs, and careful interpretation. They also depend heavily on the assumptions built into them. If the input data are weak, if important biological processes are poorly described, or if the model is stretched beyond what it has been shown to support, the output may look precise without being truly reliable.
This is why a poorly built PBPK model is not inherently better than a sensible allometric estimate. More detail is not the same as more truth. In development work, false confidence is often more dangerous than acknowledged uncertainty. The real issue is not whether a method is simple or advanced. It is whether the method matches the decision.
A practical way to think about the choice
In real programs, the choice between allometry and PBPK becomes clearer when it is framed around purpose rather than preference.
Allometric scaling is often useful when:
- the team needs an early estimate of likely human PK from animal data
- the question is still relatively straightforward
- plasma PK is the main focus
- a quick translational starting point is needed
PBPK is often useful when:
- physiology is central to the question
- tissue exposure matters
- the program needs to think through DDI risk
- the team must assess likely behavior in special populations
- dose prediction needs to integrate several different kinds of information in one framework
Seen this way, the two approaches are not fighting for the same role. They are often answering different levels of question.
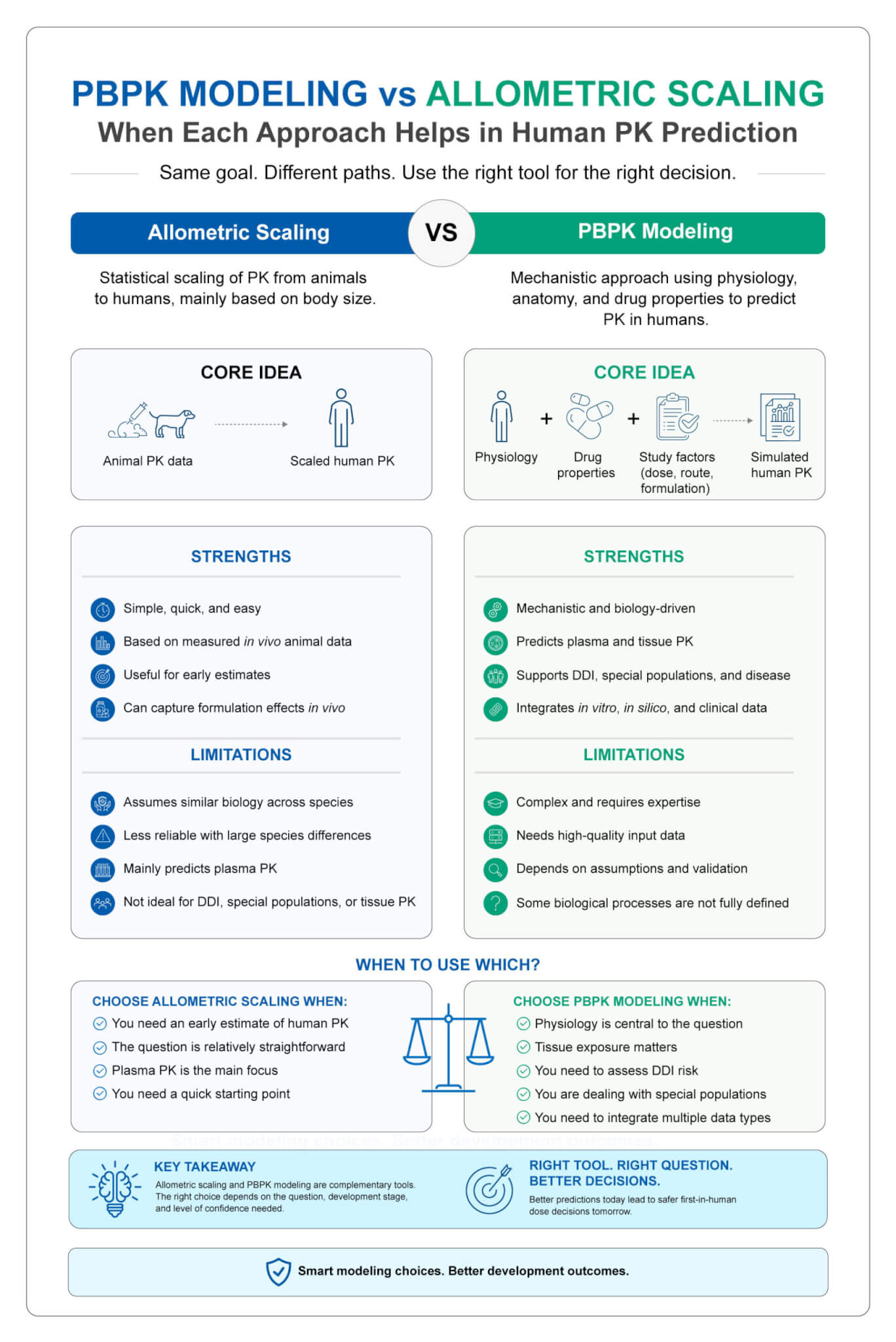
Figure 1. Allometric scaling and PBPK support human dose prediction through different approaches, helping teams select the most appropriate strategy for drug development decisions.
Why the best programs use both allometric scaling and PBPK
In practice, strong development teams do not always treat allometry and PBPK as either-or choices. Allometric scaling may provide a useful first estimate or a reality check. PBPK may then add depth where the biological question demands it. A program may begin with a simpler translational view and later move toward a more mechanistic framework as the stakes rise and the questions become more specific.
A mixed approach is often the more sensible path forward for predictions. Early development rarely benefits from unnecessary complexity. At the same time, programs moving toward the clinic cannot afford to stay with a broad scaling estimate when the real question has become physiological, tissue-specific, or interaction-driven. The value lies in knowing when to stay simple and when to go deeper.
Looking ahead
Allometric scaling and PBPK both have a legitimate place in human dose prediction, but they are useful for different reasons. Allometry is practical, familiar, and grounded in measured in vivo data. It works well when a team needs an early estimate and the translational question is relatively narrow. PBPK adds value when the question becomes more biologically demanding and when physiology, tissue exposure, DDI risk, or special populations need to be considered directly.
The best choice is one that fits the scientific and development decision in front of the team. This is what makes this comparison worth getting right. Human dose prediction is not only about selecting a method. It is about choosing the right level of thinking for the stage the program has reached.