




Why first-in-human dose decisions matter so much
PBPK modeling has become important in early drug development because few decisions carry as much weight as the first dose taken into human studies. If the first-in-human dose is too high, the risk is immediate and obvious. Participants may be exposed to avoidable safety issues, and the program may face early setbacks that could have been prevented. If the starting dose is too low, the study may produce weak or confusing data, with exposure that is insufficient to show a meaningful signal. Neither situation helps a development program move forward with confidence.
This is why first-in-human dose selection is never just a mathematical exercise. It is one of the earliest points at which scientific judgment, translational understanding, and development strategy come together in a very practical way. The chosen dose and regimen shape not only participant safety, but also the quality of the data that follow, the clarity of early decision-making, and the confidence with which a program moves into the clinic.
For this reason, human PK prediction has become a central part of early development planning. It helps teams estimate likely human exposure before clinical data exist, compare different development scenarios, and reduce the risk of avoidable mistakes at a stage where uncertainty is still high but the consequences of error are already serious.
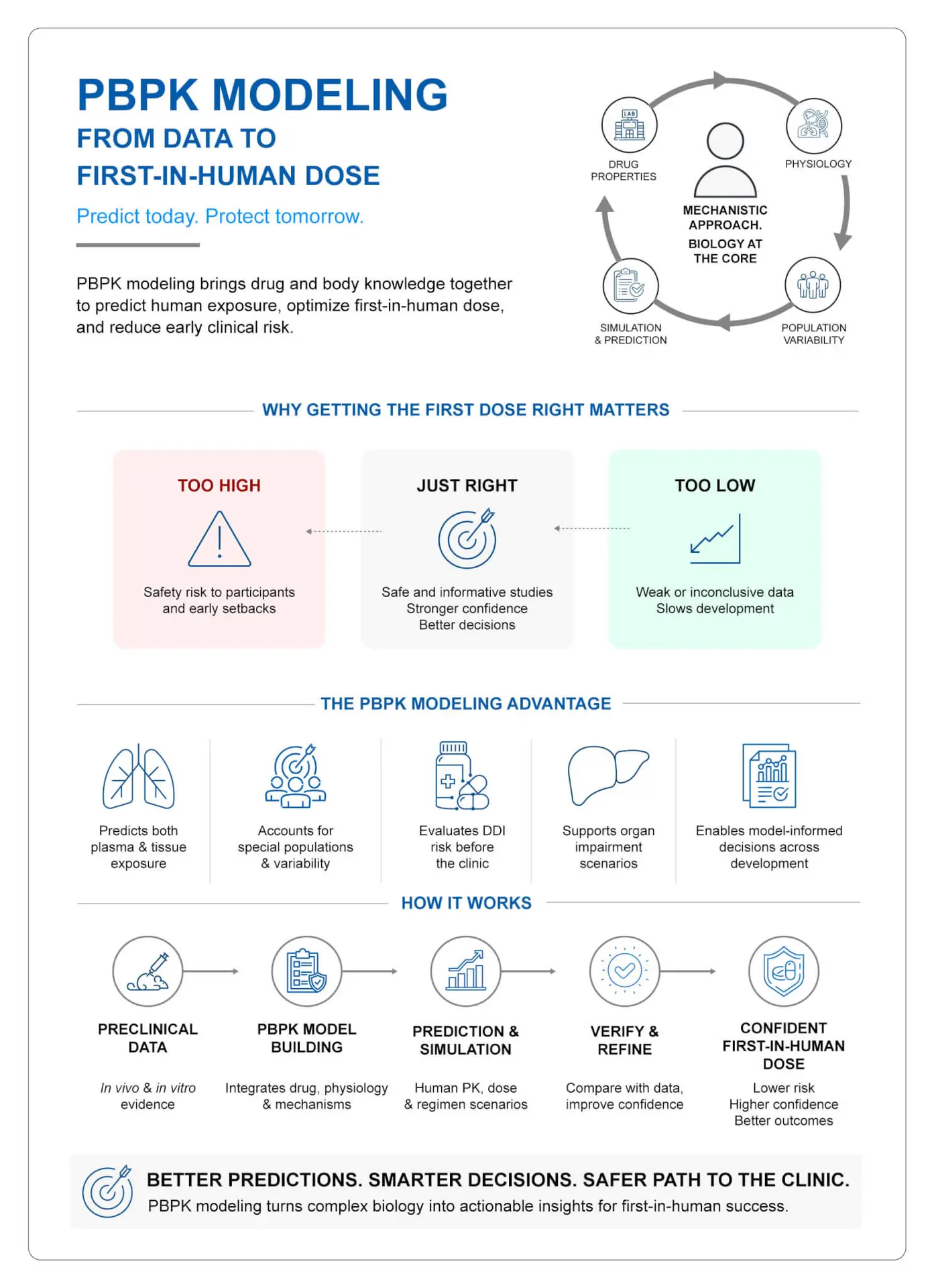
Figure 1. How PBPK modeling supports human PK prediction and first-in-human dose selection to reduce early clinical risk.
Why human PK prediction is central to early development
The purpose of human PK prediction is straightforward: to help teams make better decisions before entering the clinic. In practice, that means choosing a dose and dosing schedule that are more likely to be both safe and informative. It also means supporting broader development decisions, such as selecting the right molecules, interpreting preclinical PK-PD relationships more carefully, and strengthening animal-to-human extrapolation. In other words, PK prediction is not sitting in isolation. It influences how early evidence is translated into a clinical strategy.
The real value lies in avoiding two common but costly errors. The first is over-prediction, where expected human exposure is underestimated and the starting dose ends up being too aggressive. The second is under-prediction, where the chosen dose is so conservative that the study struggles to generate useful information. Both situations can slow a program, weaken confidence, and complicate the next phase of work.
Dose selection also becomes more complicated when multiple-dose regimens are involved. A compound that appears manageable after a single administration may behave very differently once accumulation, dose frequency, and exposure over time begin to matter. This is why teams increasingly need a more thoughtful and predictive view of human PK early in development, rather than relying only on broad assumptions or late-stage corrections.
For sponsors, the benefit is clear. Better early prediction can support a more rational clinical entry strategy, improve study design, and create a stronger basis for interpreting emerging data. For a CDMO working closely with development programs, this is where predictive DMPK begins to make a real commercial and scientific difference.
Moving from descriptive PK to a mechanistic approach
Traditional pharmacokinetic models remain useful, but they answer only part of the question. Classical empirical PK models are good at describing observed behavior. They summarize what happened in a study and help organize the data into interpretable parameters such as clearance and volume of distribution. This remains valuable. But these models are less suited to questions that go beyond the observed situation. They do not always explain why a drug behaves the way it does, and they are limited when the next question involves a different physiological state, a special population, a complex dosing scenario, or tissue-level exposure.
This is where physiologically based pharmacokinetic, or PBPK modeling, becomes useful. PBPK is a mechanistic approach. Instead of treating the body as a simplified set of empirical compartments, it represents actual organs and tissues and connects drug behavior to known physiology and compound-specific properties. This makes it possible to move from simply describing observed PK to exploring how a drug may behave under different biological or clinical conditions.
This shift matters in development. A team may initially want to know what happened in a preclinical study, but soon the more relevant question becomes what may happen in humans, in organ impairment, in children, in the presence of an interacting drug, or in a tissue that matters for efficacy or safety. Those are not minor extensions of the same question. They require a framework that can work with physiology rather than around it.
Where allometry still helps and where PBPK adds more value
Allometry continues to play an important role in dose prediction, and it remains a familiar part of development planning. In simple terms, allometry scales PK parameters across species, usually on the basis of body size or body weight. It uses observed in vivo data from animal studies and applies scaling relationships to estimate likely human values. This makes it attractive because it is relatively simple, practical, and grounded in real preclinical measurements.
This simplicity, however, is also its limitation. Allometry assumes that the biological processes driving PK are sufficiently comparable across species for the scaling to hold. It can be useful for estimating plasma PK, and in some cases, it may capture formulation-related effects better than a purely in vitro or in silico approach. But it does not offer the same mechanistic depth as PBPK. It does not readily explain tissue distribution, physiology-driven variability, transporter effects, organ-specific behavior, or the impact of altered biology in special populations.
PBPK modeling takes a different route. Instead of scaling mainly by size, it builds predictions from anatomy, physiology, and compound behavior. This gives it a broader and often more informative role when the development question is more complex.
This does not mean one approach should replace the other in every program. In reality, both can be useful. Allometry can provide a useful anchor from measured in vivo data, while PBPK can help answer the more mechanistic questions that arise as programs move closer to the clinic. What matters most is not choosing one tool by habit, but choosing the right tool for the decision at hand.
What PBPK modeling actually does in model-informed drug development
PBPK can sound more complicated than it is. At its core, it is a structured way of combining what is known about the drug with what is known about the body. A PBPK model may include organ volumes, tissue composition, blood flow, surface area, enzyme and transporter expression, physicochemical properties such as lipophilicity, ionization, and protein binding, as well as factors linked to formulation, dose, route, and regimen. It can also account for demographic and genetic variability, which makes it possible to simulate virtual populations rather than relying on a single “average” subject.
That makes the model useful because development questions rarely depend on one factor alone. Exposure is not shaped only by the chemistry of the molecule. It is also influenced by absorption, distribution, metabolism, elimination, transport, route of administration, formulation behavior, and the physiology of the person receiving the drug. PBPK modeling brings those elements together in one framework.
Plasma exposure tells only part of the story
One of the strongest advantages of PBPK is that it is not restricted to plasma PK. In many development settings, plasma exposure is an acceptable starting point. But in others, it is not enough. Teams may need to understand what is happening in target tissues, in organs linked to safety risk, or in compartments where efficacy depends on local exposure rather than systemic concentration alone.
PBPK offers a way to estimate that tissue-level behavior. For compounds where the site of action matters, or where organ-specific toxicity is a concern, this added layer of understanding can materially improve development decisions. It also helps move the conversation from broad exposure estimates toward more biologically relevant interpretation.
Strong models still depend on strong assumptions
PBPK is a powerful approach, but it should not be treated casually. These are complex models that require expertise, good-quality inputs, and careful interpretation. Some biological processes are still imperfectly described. Some parameter values are uncertain. In vitro systems do not always reflect in vivo conditions perfectly. Validation remains critical, especially when a model is expected to support an important development or regulatory decision.
This is why the real strength of PBPK is not that it removes uncertainty. Its strength is that it makes uncertainty more visible, more testable, and more manageable. It gives teams a more disciplined way to ask whether their assumptions are scientifically reasonable before those assumptions become expensive in the clinic.
Why iterative PBPK modeling matters
The most useful PBPK work is rarely a one-time prediction. In well-run programs, modeling becomes part of an iterative process. A model may begin with animal data, in vitro findings, and compound-specific properties. Those predictions are then compared with observed results. If the agreement is reasonable, the model can be carried forward into healthy volunteer simulations and then into more specific patient populations. If the agreement is weak, the right response is not to force confidence into the model. It is to revisit the assumptions, gather additional information where needed, and refine the framework.
This learn-confirm-refine pattern is one of the most practical reasons PBPK modeling is so valuable. It mirrors how good development decisions are actually made. Programs improve when teams test their assumptions early, confront mismatches honestly, and use each round of evidence to strengthen the next decision.
For a CDMO, this iterative mindset is especially important. Clients do not only need data or software output. They need support in connecting multiple layers of evidence, understanding where uncertainty still sits, and translating that understanding into better development choices.
A practical example: using PBPK to assess DDI risk
The value of PBPK becomes much easier to appreciate when it is linked to a practical problem. Drug-drug interactions are one such problem. They are common, important, and often difficult to assess with confidence using simple assumptions alone. A mechanistic model can help teams estimate the likely effect of metabolic enzymes, transporters, and co-administered inhibitors before those questions are fully explored in the clinic.
A useful example is the application of PBPK to repaglinide, a short-acting antidiabetic drug. In this case, the model brought together compound-specific properties and mechanistic assumptions to evaluate the contribution of CYP2C8, CYP3A4, and OATP1B1 to drug disposition. Simulations with trimethoprim, clarithromycin, and cyclosporine were then used to estimate the effect of different inhibitors on exposure.
The value was not only in generating predictions. It was in comparing those predictions with observed data and seeing whether the model captured the interaction pattern with reasonable accuracy. When predicted and observed exposure changes align well enough, confidence in the model improves. This, in turn, strengthens the basis for exploring more complicated interaction scenarios.
This kind of work is highly relevant to early development. It allows teams to think about interaction risk before the problem becomes a clinical complication. It also creates a clearer link between mechanistic understanding and dose strategy, rather than leaving DDI assessment as a late-stage reactive exercise.
Why PBPK matters in special populations
Few areas show the practical value of PBPK more clearly than special population strategy. Development does not stay within the boundaries of the healthy average adult for long. Teams often need to consider what may happen in children, older adults, pregnant patients, or individuals with hepatic or renal impairment. Physiology changes across these groups in ways that may materially affect exposure, dose, and risk.
PBPK provides a framework for exploring those differences more systematically. Because the model is built on physiology, it can incorporate altered organ size, blood flow, enzyme activity, transporter expression, and disease-related changes that affect drug disposition. This makes it especially useful where direct clinical evidence is limited, difficult to obtain, or ethically sensitive.
This does not mean modeling replaces evidence. It means modeling helps make better use of the evidence that already exists and helps define where additional evidence is most needed. In some situations, it may support dose reasoning strongly enough to reduce the need for certain studies or to guide the design of those studies more effectively.
For sponsors, this can save time and improve clarity. For development partners, it offers a more thoughtful way to support clinically relevant decision-making in populations where uncertainty is naturally higher.
Why model-informed drug development is changing regulatory thinking
PBPK is no longer treated as a niche scientific exercise. Over the past several years, it has become increasingly visible in model-informed drug development and in regulatory submissions. Its use in areas such as DDI assessment, dose selection, organ impairment, pediatrics, and other special populations has grown steadily. Regulatory agencies have also shown increasing interest in frameworks that support model credibility, reduced reliance on animal testing, and better use of mechanistic evidence in development decisions.
This matters because it changes how modeling should be viewed inside development programs. PBPK is not something to consider only after a difficult question appears. It is increasingly part of how teams prepare for those questions in advance.
For a CDMO, this shift is significant. It means that translational and modeling capabilities are not simply technical add-ons. They are part of a broader readiness package that supports better dose rationale, stronger clinical planning, and more confident development discussions.
What PBPK modeling means for sponsors approaching first-in-human studies
The practical message is simple. Early clinical risk is not driven only by toxicology findings or operational gaps. It is also shaped by how well a program understands likely human exposure before the clinic begins. Programs can lose time and momentum when dose assumptions are weak, interaction risk is poorly understood, or variability across populations is treated too late. Predictive DMPK helps reduce those blind spots. PBPK modeling is one of the most useful tools in that effort because it connects discovery data, preclinical understanding, physiology, and clinical questions in one structured framework. Used well, it helps teams enter the clinic with a stronger rationale, a clearer view of uncertainty, and a more defensible dose strategy. This is why its value extends beyond modeling itself. It supports better judgment for development.
Closing perspective
First-in-human dose selection is one of the earliest and most important tests of development thinking. The question is not only how much drug to give. The deeper question is how well a program understands likely human exposure before that first decision is made. PBPK helps answer this question more thoughtfully by combining drug-specific properties with physiology, supporting DDI assessment, extending reasoning into special populations, and bringing more structure to early translational decision-making.
It is not a shortcut, and it is not a replacement for scientific judgment. Its value lies in making this judgment better informed. For development teams working toward the clinic, this can make a real difference. In a setting where early errors can be costly and difficult to unwind, predictive DMPK helps reduce avoidable risk and supports a stronger path forward.