




Introduction
A drug that performs perfectly in the lab can still fail with a real patient if it is not taken the way it was designed to be taken. At CPHI North America 2026, Vivek Kumaravel, Associate Vice President at Syngene International, walked through how Syngene’s formulation team solves this problem in oral solid dosage development, backed by real case studies on pharmacokinetic variability, food effect and pill burden. Watch the full session as an on-demand webinar or read on for the key takeaways.
Why Bioavailability Alone Isn’t Enough
Bioavailability is only part of the equation in oral solid dosage form development. Drugs carry inherent pharmacokinetic variability between and within patients, driven by the drug substance, GI physiology and the formulation. Many also show a food effect, where the same dose behaves differently fasted versus fed, while high dose burden and difficulty swallowing add further strain for pediatric and geriatric patients. All of this shows up as inconsistent adherence, and a formulation that solves bioavailability on the bench but ignores how it is taken has not solved the real problem.
How Syngene Selects the Right Drug Delivery Platform
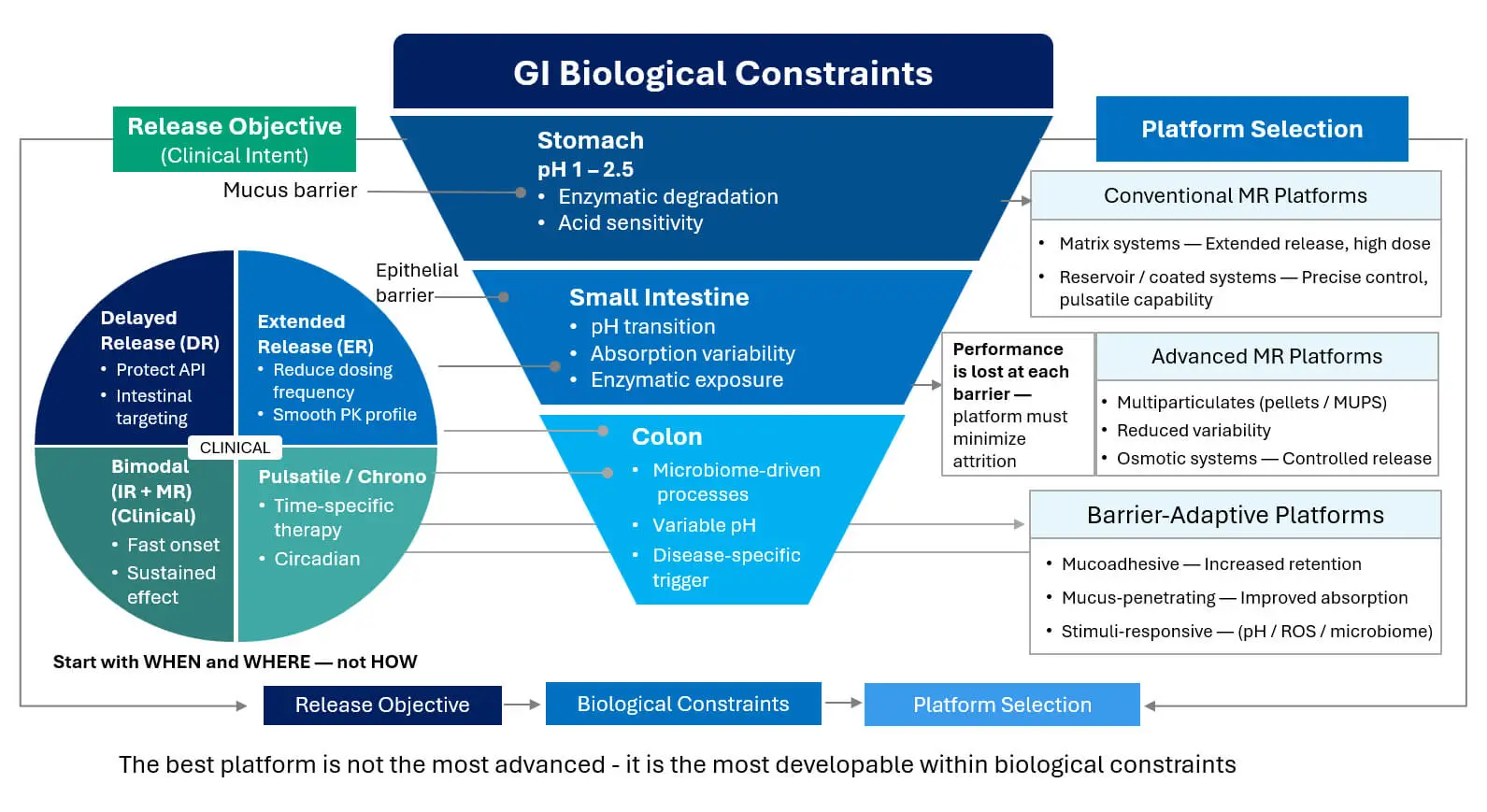
Before choosing a delivery technology, Syngene’s team first defines clinical intent: when and where the drug needs to release, whether that calls for delayed release, extended release or a chronotherapeutic profile. That decision has to respect the GI tract’s barriers, including pH shifts, enzymes, mucus and the microbiome, since each segment of the gut behaves differently. An acid-labile drug, for example, needs delayed release to avoid degrading in the stomach, while a drug metabolized lower in the intestine may need a gastro-retentive system instead. Platform selection has to be physiology-driven, not technology-driven.
A Data-Driven Way to Manage Pharmacokinetic Variability
Pharmacokinetic variability cannot be eliminated, only understood and designed around, and solubility is usually the first barrier a molecule has to clear. Syngene uses a developability classification system (DCS) that plots solubility against permeability and sorts molecules into four categories. Highly soluble, highly permeable molecules need little more than a simple solution. Molecules limited by dissolution rate respond to particle size reduction or disintegrants. Poorly soluble molecules need an amorphous solid dispersion, built through spray drying or hot melt extrusion, to stay supersaturated. The hardest molecules, limited by permeability, call for permeation enhancers or lipid-based carriers.
Two Formulation Case Studies: Solving Food Effect and Pill Burden
In one project, an antipsychotic carried a boxed warning requiring patients to take it with food, a real adherence risk for a population already managing a psychotic disorder. Syngene’s team traced the issue to pH-dependent solubility: the drug dissolved well in the acidic stomach but precipitated out in the intestine’s higher pH. The fix was a pH-sensitive amorphous dispersion that limited release in acid and kept the drug supersaturated in the intestine, bringing fasted and fed exposure within the standard 80 to 125 percent bioequivalence range.
In another, a cardiovascular treatment dosed three times a day needed to become once daily, but its active metabolite had a half-life of roughly 80 hours against the parent compound’s one hour, risking toxic accumulation if release was slowed too much. Using PBPK modeling, Syngene’s team found a dissolution window that balanced exposure against metabolite buildup and combined dose fractionation with upper GI targeting to limit it further. The reformulated product is now in clinical testing.
Designing for Swallowability and Patient Adherence
Swallowability gets its own attention: taste masking for pediatric patients, easier-to-swallow formats for geriatric patients, and tools like orally disintegrating tablets, chewables and multiparticulates for both. Kumaravel also touched on chronotherapeutics, timing release for conditions like rheumatoid arthritis so drug levels peak with morning symptoms, through a dual-pulse release built with pH-triggered coatings. Every example relied on biorelevant, stress-tested dissolution methods rather than standard testing alone, since that is what predicts real-world performance.
Frequently Asked Questions
Why do some oral drugs need to be taken with food? Because solubility depends on pH. A drug can dissolve in the stomach’s acid but precipitate out in the more neutral intestine unless food changes that environment.
How can a three-times-daily drug become a once-daily formulation? By using PBPK modeling to find a dissolution rate that delivers enough parent drug without letting a long-lived metabolite build up to unsafe levels.
What is chronotherapeutics in drug formulation? An approach that times release to match a patient’s symptom pattern, such as releasing most of a dose hours after a nighttime tablet so levels peak with morning symptoms.
Watch the Full On-Demand Webinar
This is only a snapshot. The on-demand webinar covers the full reasoning behind each case study, including the dissolution data, the PBPK modeling and the testing strategy that got each formulation right. Watch it here.